Koa Mindset for Depression. From 15% to 95% shared components — unifying a fragmented design system.
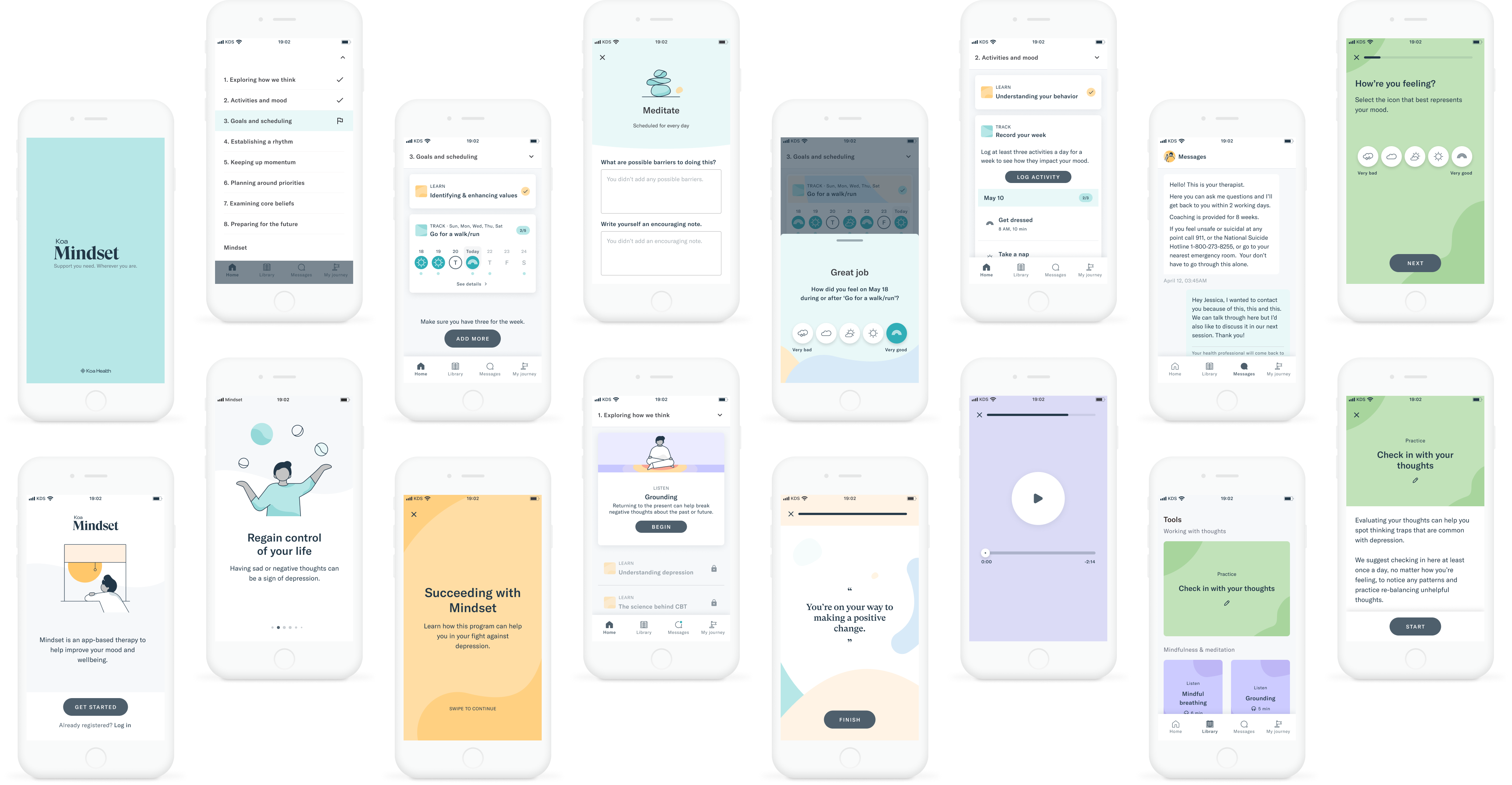
Overview of Koa Mindset after using Design System components
In 2022, I audited Koa Mindset's design against Koa Health's other live product, Koa Foundations, surfacing where each had drifted into custom components and divergent patterns — and raising specific gaps and needs to the Design System team. Both products had accumulated bespoke solutions, creating inconsistencies for users, duplicated code for engineers, and no clear path to design system adoption. That audit became the case for a formal standardization initiative, which I helped lead alongside the Design System lead and engineering — replacing components bottom-up, view by view, without a feature freeze, to increase shared component usage across both products. We moved from roughly 15% to 95% shared components, removed over 150 custom components, and shipped a product that went on to achieve a 4.3/5 quality rating and 7% dropout rate in a peer-reviewed clinical trial.