Koa Mindset for Depression. A CBT-based mental health app validated in a Harvard clinical trial.
Mindset for Depression — 8-week CBT programme for adults with major depressive disorder
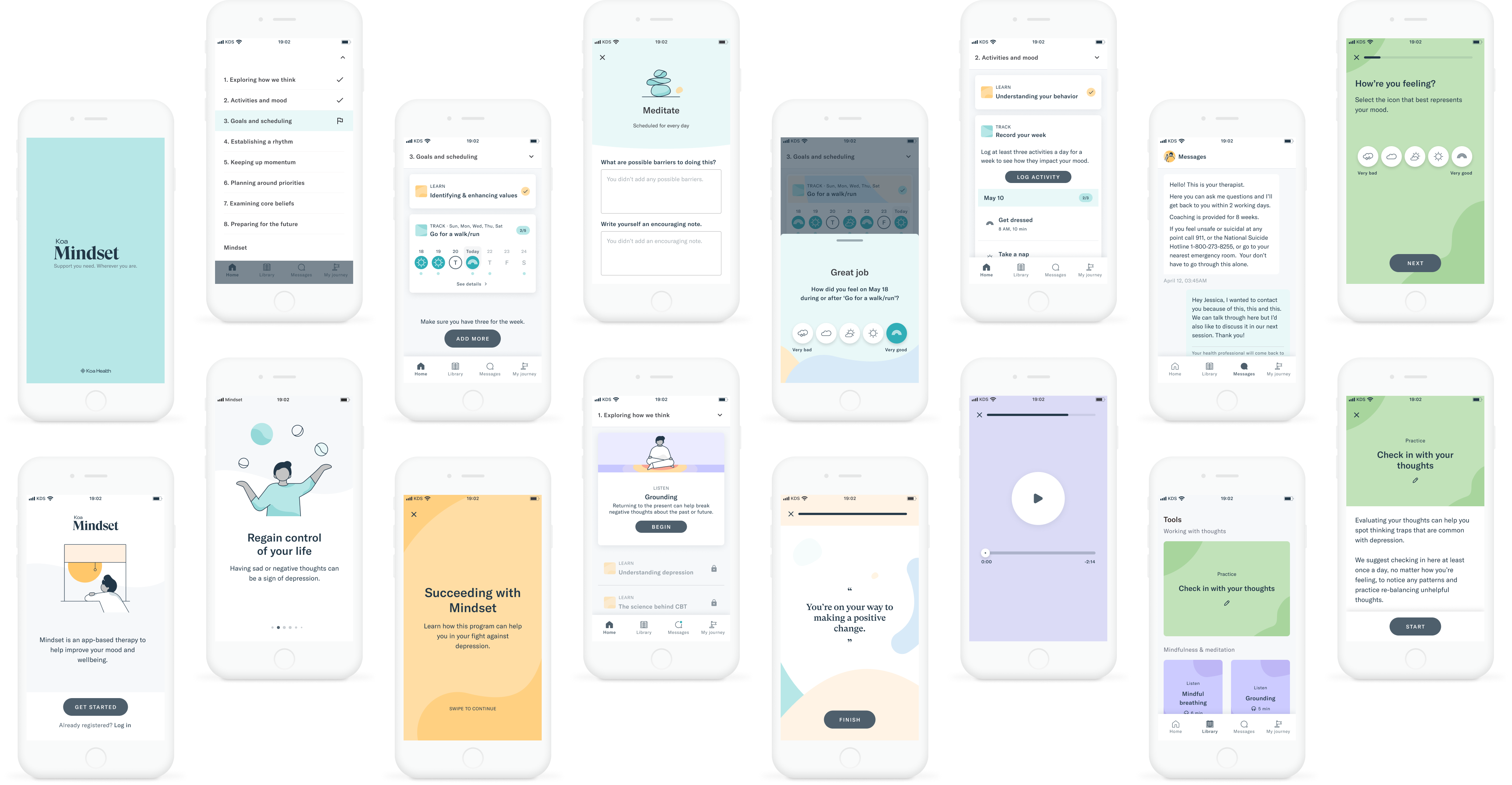
In 2022, I worked on Mindset for Depression, a CBT-based mental health app developed by Koa Health in collaboration with Massachusetts General Hospital and Harvard Medical School. The aim was to make a full course of cognitive behavioural therapy accessible through a smartphone, enabling licensed therapists to focus their clinical time on personalisation and safety monitoring rather than re-explaining foundational content. This involved designing the interaction patterns and activity flows for each of the 8 clinical steps, revamping the logging experience to reduce friction on a behaviour users needed to complete repeatedly, and designing safety check-ins that could account for suicidal ideation without blocking access to the content that might help. The product was tested in a peer-reviewed open trial, achieving a large effect size for depression severity reduction (d=1.47), a 7% dropout rate across 8 weeks, and an 82.7% homework completion rate — with the published paper explicitly attributing part of the product's success to the design approach.